Poster
1 Page
Preview
Page 1
smartsigns Patient Monitoring
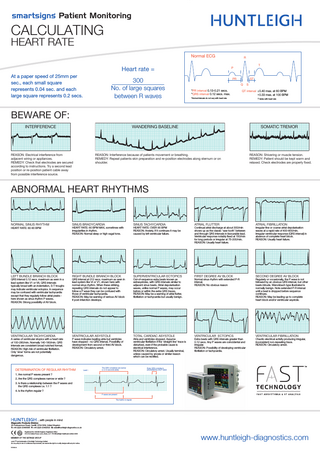
CALCULATING HEART RATE
Normal ECG
Heart rate = At a paper speed of 25mm per sec., each small square represents 0.04 sec. and each large square represents 0.2 secs.
300 No. of large squares between R waves
R T
P
PR
ST Q
*PR interval 0.13-0.21 secs. *QRS interval 0.12 secs. max.
S
QT interval † 0.40 max. at 60 BPM † 0.33 max. at 100 BPM
*Normal intervals do not vary with heart rate
† Varies with heart rate
BEWARE OF: INTERFERENCE
WANDERING BASELINE
REASON: Electrical interference from adjacent wiring or appliances. REMEDY: Check that electrodes are secured according to instructions. Try a second lead position or re-position patient cable away from possible interference source.
SOMATIC TREMOR
REASON: Interference because of patients movement or breathing. REMEDY: Repeat patients skin preparation and re-position electrodes along sternum or on shoulder.
REASON: Shivering or muscle tension. REMEDY: Patient should be kept warm and relaxed. Check electrodes are properly fixed.
ABNORMAL HEART RHYTHMS
NORMAL SINUS RHYTHM
SINUS BRADYCARDIA
SINUS TACHYCARDIA
ATRIAL FLUTTER
ATRIAL FIBRILLATION
LEFT BUNDLE BRANCH BLOCK
RIGHT BUNDLE BRANCH BLOCK
SUPERVENTRICULAR ECTOPICS
FIRST DEGREE AV BLOCK
SECOND DEGREE AV BLOCK
VENTRICULAR TACHYCARDIA
VENTRICULAR ASYSTOLE
TOTAL CARDIAC ASYSTOLE
VENTRICULAR ECTOPICS
VENTRICULAR FIBRILLATION
HEART RATE: 60-90 BPM
QRS interval 0.12 secs. maximum as seen in a lead system like V1 or V6. QRS intervals typically broad with an indentation, S-T troughs may indicate ventricular ectopics. In sequence may be confused with ventricular tachycardia except that they regularly follow atrial peaks here shown as sinus rhythm P waves. REASON: Strong possibility of AV block.
A series of ventricular etopics with a heart rate of 100-280/min. Normally 140-180/min. QRS intervals are consistent broad notched format. REASON: High risk of ventricular fibrillation. Only ‘slow’ forms are not potentially dangerous.
HEART RATE: 60 BPM MAX, sometimes with irregularities in rhythm. REASON: Normal sleep or high vagal tone.
QRS interval at 012 secs. maximum as seen in lead system like Vr or V1, shown here with normal sinus rhythm. When these striking, repeating QRS intervals do not appear to follow a P wave they can be confused with those of ventricular tachycardia. REASON: May be warning of serious AV block if post-infarction develops.
P wave indicates beating atria but ventricles have stopped - no QRS interval. Possibility of development from second or third AV block. REASON: Circulatory arrest.
DETERMINATION OF REGULAR RHYTHM
Lead I
The QRS complexes are narrow (< 0.12 seconds wide)
HEART RATE: OVER 90 BPM REASON: Anxiety. If it continues it may be caused by left ventricular failure.
Out-of-sequence extra beats known as extrasystoles, with QRS intervals similar to adjacent sinus beats. Atrial depolarisation waves, unlike normal P waves, may occur before or within the extra QRS traces. REASON: May be a warning of atrial flutter, fibrillation or tachycardia but usually benign.
Atria and ventricles stopped. Assume ventricular fibrillation if the ‘straight line’ trace is disturbed, even if the probable cause is electrical interference. REASON: Circulatory arrest. Usually terminal, unless caused by anoxia or similar reason which can be rectified.
Continual atrial discharge at about 300/min shows up as the classic ‘saw tooth’ between and through QRS intervals in favourable lead. Ventricular response notably fixed at 150/min for long periods or irregular at 75-200/min. REASON: Usually heart failure.
Normal sinus rhythm with extended P-R interval. REASON: No obvious reason
Extra beats with QRS intervals greater than 0.12 secs. Any P waves are coincidental and irregular. REASON: Possibility of developing ventricular fibrillation or tachycardia.
Irregular fine or coarse atrial depolarisation waves at a rapid rate of 400-600/min. Irregular ventricular response (QRS interval) in absence of complete heart block. REASON: Usually heart failure.
Regularly or occasionally, the P wave is not followed by an obvious QRS interval, but other beats intrude. Wenckbach type illustrated is normally benign. Note extended P-R interval until a beat is dropped before sequence continues. REASON: May be leading up to complete heart block and/or ventricular asystole.
Chaotic electrical activity producing irregular, inconsistent non-repeating trace. REASON: Circulatory arrest.
Every QRS complex is preceeded by one P wave
1. Are normal P waves present ? 2. Are the QRS complexes narrow or wide ? 3. Is there a relationship between the P waves and the QRS complexes i.e. 1:1 ? 4. Is the rhythm regular ? P waves are present The rhythm is regular
…with people in mind Diagnostic Products Division 35 Portmanmoor Road, Cardiff, CF24 5HN, United Kingdom T: +44 (0)29 20485885 F: +44 (0)29 20492520 E: [email protected] Registered No: 942245 England. Registered Office: 310-312 Dallow Road, Luton, Beds, LU1 1TD ©Huntleigh Healthcare Limited 2008
MEMBER OF THE GETINGE GROUP ® and ™ are trademarks of Huntleigh Technology Limited As our policy is one of continuous improvement, we reserve the right to modify designs without prior notice.
747469-A
www.huntleigh-diagnostics.com